 PeteFree.com
PeteFree.comFor males 12 to 40 — myocarditis risk from 2nd dose Moderna vaccine — is greater than myocarditis risk posed by SARS-CoV-2
© 2021 Peter Free
16 December 2021
Somebody finally looked at COVID vaccine data
Receiving a second dose of Moderna's (mRNA-1273) COVID-19 vaccine may be medically riskier to some demographics — than falling ill with SARS-CoV-2 itself.
Below is Figure 2 from a recent British study that compared, among other things, the risk of developing myocarditis after receiving anti-COVID vaccines — versus — the risk of developing myocarditis from SARS-CoV-2 infection itself.
Here is a portion of Figure 2 from their article and the authors' explanation of it:
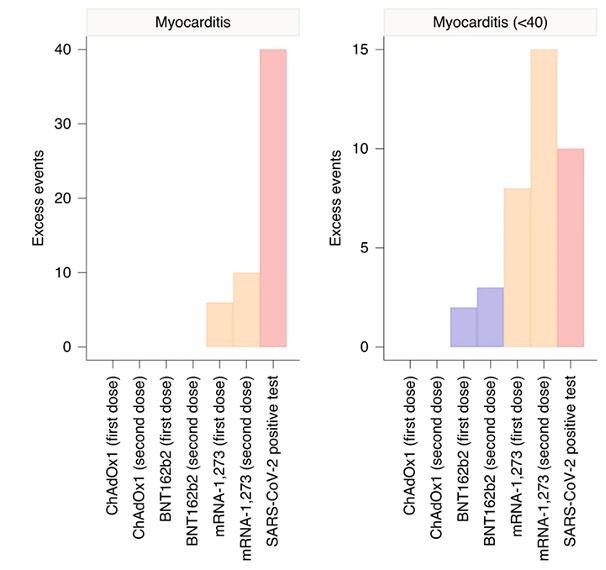
Subgroup analyses by age showed that the increased risk of events associated with the two mRNA vaccines was present only in those aged under 40 years.
For this age group, we estimated 2 . . . and 8 . . . excess cases of myocarditis per 1 million people receiving a first dose of BNT162b2 [Pfizer] and mRNA-1273 [Moderna], respectively, and 3 . . . and 15 . . . excess cases of myocarditis per 1 million people receiving a second dose of BNT162b2 and mRNA-1273, respectively.
This compares with ten . . . extra cases of myocarditis following a SARS-CoV-2 positive test in those aged under 40 years.
© 2021 Martina Patone, Xue W. Mei, Lahiru Handunnetthi, Sharon Dixon, Francesco Zaccardi, Manu Shankar-Hari, Peter Watkinson, Kamlesh Khunti, Anthony Harnden, Carol A. C. Coupland, Keith M. Channon, Nicholas L. Mills, Aziz Sheikh and Julia Hippisley-Cox, Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection, Nature Medicine, https://doi.org/10.1038/s41591-021-01630-0 (14 December 2021) (showing portion of Figure 2, at PDF page 11)
The second graph . . .
. . . (on the right side of Figure 2) shows the study's findings for people aged 12 to 40.
And the fourth bar (in that second graph) shows the risk of developing myocarditis — after receiving Moderna's second dose of COVID-19 vaccine — as compared to people with myocarditis that was presumably caused by SARS-CoV-2, absent any COVID vaccine.
Interpretation
Obviously, the age 12-40 Moderna myocarditis bar is taller than the non-vaccine myocarditis bar.
That means that the risk of:
(a) developing myocarditis after Moderna's second COVID vaccine dose is
(b) noticeably greater than not getting Moderna's second dose and suffering potential myocarditis from the infective disease.
Although the absolute risk for myocarditis — 'absolute' meaning 'real' numbers of people affected — is roughly only 15 per million vaccinated folks — as opposed to the unvaccinated 10 from COVID-19 — the relative risk is quite notably 50 percent higher.
This is not what vaccines are supposed to do. At least not in any rationally sane society.
It gets worse — the data, as presented, are potentially misleading
The study did not separate the 12 to 40 group into narrower age segments.
Nor did it distinguish between men and women.
Those two attributes mean that the risk of second dose Modenra-associated myocarditis — in men aged 12-40 — is probably even greater than the magnitude displayed by the tallest bar in Figure 2.
This is because previous studies have demonstrated that men are substantially more at risk for COVID vaccine-related myocarditis than women are.
Specifically, the above-quoted British study (probably inadvertently) dilutes its most concerning finding by watering down the at-myocarditis-risk group with a large clump of mostly unaffected women.
Similarly, the study's authors have — and cannot have — any idea what the actual rate of myocarditis was among unvaccinated people, who developed unreported and untested COVID.
It is entirely possible (and probably very likely) that myocarditis shows up at much lower rates in SARS-COV-2-infected people overall, than anyone recognizes.
The assumption that myocarditis rate in ill and tested people is comparable to those who are not ill (or less ill) is probably wrong. One would expect less ill, non-reporting people not to be experiencing especially noticeable rates of myocarditis.
If that is true, it would further elevate the comparative risk of developing myocarditis from the second Moderna injection — in men 12-40 — as compared to their myocarditis risk due only to SARS-CoV-2 infection.
In summary, this study — through no fault of its authors, given the exigencies of the data collection they had to deal with — waters down the myocarditis risks of the second dose of Moderna vaccine (in men) — as compared to the risk of developing myocarditis from SARS-CoV-2 infection.
The myocarditis risk to men (aged 12-40) is probably higher — compared to that posed by SARS-CoV-2 infection — than the above study's Figure 2 graph indicates.
The moral? — There is no medically legitimate reason to push second-dose Moderna vaccinations in younger men
Substitute Pfizer or something else.
COVID vaccine Maoism in the United States, as a form of evidence-ignoring religion, needs to face facts.
And the United States' long-demonstrated aversion to investigating virtually anything that has to do with COVID and COVID vaccines should terminate.
Ask yourselves, why obviously necessary medical investigations — like the one that the above-cited authors undertook — continue to be repressed in the United States.